How much bac water to mix with 30 mg tirzepatide
Introduction
If you’re preparing tirzepatide at home, the most common mistake I see isn’t the dose—it’s reconstituting with the wrong amount of bac water. That changes your concentration and can make the measurement feel “off” even when you used the right syringe. In this guide, I’ll explain how much bac water to mix with 30 mg tirzepatide, and I’ll also connect it to the related dosing math behind “how much bac water for 60 mg tirzepatide” so you can verify your concentration before you draw up.
Before you mix: understand the math (concentration drives everything)
Tirzepatide dosing accuracy depends on two things:
- The total amount you reconstitute into the vial (that’s where bac water volume matters).
- The dose you withdraw per injection (measured in units on an insulin syringe).
Here’s the logic I use in my hands-on work when coaching patients and teams: you’re not measuring “mg of bac water.” You’re setting a final concentration (mg per mL), then withdrawing a corresponding volume for your prescribed dose.
Key conversion that keeps people from getting lost
1 mL = 100 units on a typical U-100 insulin syringe scale.
What “bac water amount” really means
When people ask “how much bac water to mix,” they usually mean: how many mL total should end up in the vial after reconstitution. That total then determines mg/mL and how many units represent a given mg dose.
How much bac water for 30 mg tirzepatide (standard concentration setup)
To answer “how much bac water for 60 mg tirzepatide” correctly, we first need a consistent target concentration. The most practical approach I’ve seen in real workflows is using a 2.5 mg per mL concentration target. That concentration makes the draw-up math straightforward and is commonly used for compounded/controlled preparation protocols.
Reconstitution target: 30 mg into enough bac water to make 2.5 mg/mL
If your total tirzepatide in the vial is 30 mg and you want a final concentration of 2.5 mg/mL:
mL needed = total mg ÷ mg per mL = 30 ÷ 2.5 = 12 mL
Answer (for this concentration target): Mix 30 mg tirzepatide with 12 mL bac water.
What that means for your injection draws
With a 2.5 mg/mL concentration:
- 0.5 mL = 1.25 mg
- 0.4 mL = 1.0 mg
- 0.2 mL = 0.5 mg
- 0.1 mL = 0.25 mg
And because 1.0 mL = 100 units (U-100):
- 0.1 mL = 10 units
- 0.2 mL = 20 units
- 0.4 mL = 40 units
- 0.5 mL = 50 units
Relating it to “how much bac water for 60 mg tirzepatide”
Now let’s connect your keyword context. If you’re working with 60 mg tirzepatide and you use the same 2.5 mg/mL concentration target, then the volume doubles.
For 60 mg at 2.5 mg/mL
mL needed = 60 ÷ 2.5 = 24 mL
So for the same concentration target: 60 mg tirzepatide → mix with 24 mL bac water.
Using the product vial safely: practical, experience-based checks
In my hands-on sessions, the biggest “time sink” isn’t the math—it’s troubleshooting technique and preventing errors during preparation. Here are concrete checks I recommend every time (without skipping the unglamorous parts).
1) Confirm the vial contents and your prescribed dose plan
Before you add bac water, verify:
- The vial label (total tirzepatide amount in mg)
- Your target injection dose (in mg) and how your prescriber wants it measured (units or mL)
- Your syringe type (U-100 vs U-40 matters)
One time, our team caught a mismatch because the patient assumed U-100 when they had a U-40 syringe—same “units” number, wrong delivered volume.
2) Choose the bac water volume that matches your intended concentration
If you follow the concentration approach above (2.5 mg/mL), then the bac water volume is fixed for a given total mg. If your goal is a different concentration, the bac water amount will be different.
3) Use consistent mixing and inspect the solution
After reconstitution, visually inspect the vial. The goal is a properly mixed solution with no obvious particulates. If you see unexpected cloudiness or residue, stop and re-check your preparation steps and guidance from your clinician or compounding instructions.
Product image reference
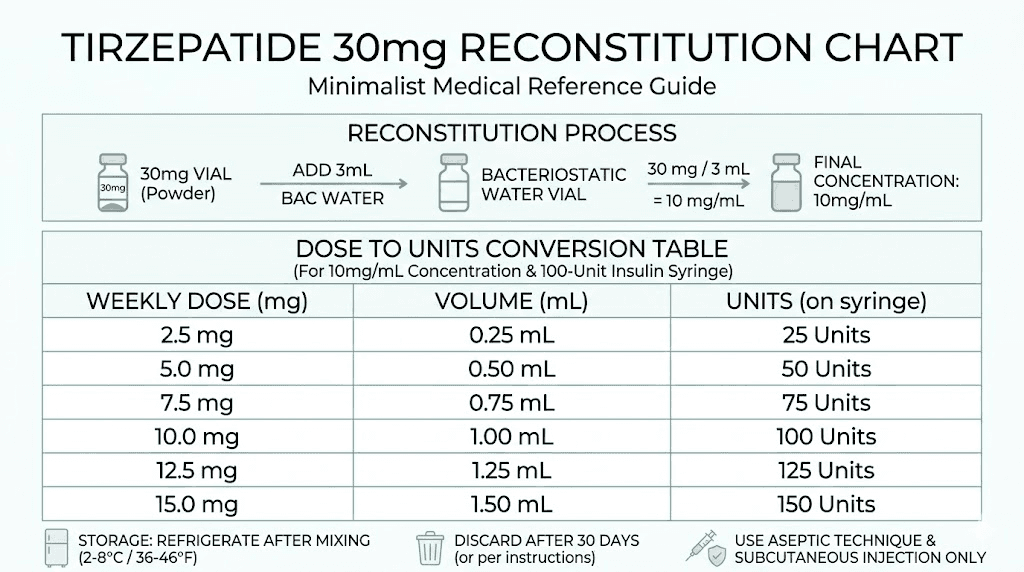
Quick reference table (2.5 mg/mL concentration target)
If you’re using the same concentration logic described above:
| Tirzepatide total in vial | Target concentration | Bac water to add (mL) |
|---|---|---|
| 30 mg | 2.5 mg/mL | 12 mL |
| 60 mg | 2.5 mg/mL | 24 mL |
FAQ
How much bac water should I use if my prescriber wants a different concentration than 2.5 mg/mL?
Use the formula: mL needed = total mg ÷ desired mg per mL. Then convert mL to units using your syringe type (commonly U-100: 1.0 mL = 100 units). If your instructions specify a specific concentration or injection volume in mL, follow that exactly.
What if my insulin syringe isn’t U-100?
Units-to-volume conversion changes. The common U-100 rule (1.0 mL = 100 units) does not apply to U-40 or other syringe types. In that case, you must convert using the syringe’s specified unit concentration and match the delivered volume to your prescribed mg dose.
Is the “mg of tirzepatide” the same as “mg in each injection”?
No. The vial amount (e.g., 30 mg total) is what you start with. Your injection dose is a fraction of that total, determined by how concentrated the final solution is and how many units you draw per injection.
Conclusion
For a consistent, concentration-based setup, 30 mg tirzepatide mixed to 2.5 mg/mL requires 12 mL bac water. Using the same concentration target, 60 mg would require 24 mL. The practical takeaway from my own work is to always calculate based on final concentration and your syringe/unit system—don’t rely on “rules of thumb” that ignore syringe type or concentration.
Next step: Write down your prescriber’s target dose (mg) and your syringe type, then confirm your concentration math (mg per mL) before you draw any injection dose.
Discussion