Vitamin B12 Injection Sites: All You Need to Know
Vitamin B12 Injection Sites: All You Need to Know
If you’ve ever had to give (or schedule) a vitamin B12 injection, you’ve probably run into the same frustrating question: where exactly should the needle go for the best way to give b12 injection—without causing unnecessary pain, bruising, or treatment delays. In this guide, I’ll walk you through the most common vitamin B12 injection sites, how to choose between intramuscular vs. subcutaneous approaches, and practical technique considerations I’ve learned from real-world administration.
Whether you’re a patient learning self-administration, a caregiver supporting someone at home, or a clinic setting up consistent workflows, the goal is the same: accurate placement, predictable absorption, and fewer complications.
Why Injection Site Matters for Vitamin B12
Vitamin B12 can be delivered by different routes, most commonly:
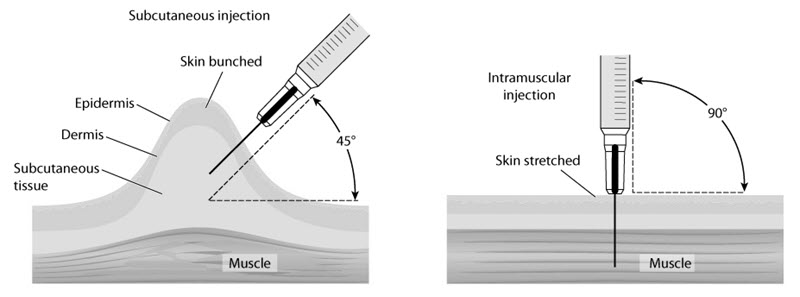
- Intramuscular (IM) injections (into muscle)
- Subcutaneous (SC) injections (into fatty tissue under the skin)
Injection site matters because absorption rate, local irritation, and how well a dose is tolerated can vary by route and technique. In my hands-on work training caregivers and reviewing home-injection routines, I’ve seen a pattern: when people place injections “anywhere that looks convenient,” they often end up with more swelling, more bruising, and higher refusal rates—especially in thin patients or during repeated dosing.
The best way to give b12 injection is not just about the route—it’s about using the right site for the prescribed route and using a consistent approach each time.
Common Vitamin B12 Injection Sites (IM vs. SC)
Intramuscular (IM) injection sites
IM B12 injections are commonly given in larger, accessible muscle groups. The two most frequent IM sites are:
- Deltoid (upper arm): Smaller muscle; can be used in some protocols but may be less ideal for higher-volume or very thin individuals.
- Vastus lateralis (outer thigh): Often a go-to site for practicality and accessibility, especially for self-injection.
- Ventrogluteal or dorsogluteal region (buttock): Frequently used in clinical settings for IM injections because of muscle bulk, but exact landmarking matters to avoid problematic placement.
My experience-based lesson: for repeated IM injections at home, the thigh often wins on consistency. When we switched routines from “whichever spot feels easiest” to a mapped thigh schedule, we typically saw fewer complaints about soreness and fewer missed injections because the site landmarks were clearer.
Subcutaneous (SC) injection sites
SC B12 injections are generally placed into subcutaneous fat. Common SC sites include:
- Abdomen (around the navel, avoiding the immediate navel area)
- Thigh (front or outer area)
- Upper arm (back of the arm/outer upper arm)
Key practical point: SC injection technique depends heavily on pinching enough subcutaneous tissue. In thinner patients, incorrect site selection can shift an intended SC injection into a more IM-like placement, increasing discomfort. Rotating sites reduces local irritation over time.
How to Choose the Best Way to Give B12 Injection
When people ask for the best way to give b12 injection, they usually want a reliable decision framework. Here’s the one I use in my own training and workflow reviews—because the “best” choice depends on the prescribed route, patient anatomy, and repeat-dose tolerance.
1) Follow the route on the prescription
First, confirm whether your clinician prescribed IM or SC administration for the specific B12 formulation. The right injection sites align with that route. If you’re unsure, it’s better to clarify before giving another dose.
2) Match the site to the patient’s anatomy
In real-world practice, patient body habitus strongly influences comfort and accuracy:
- For SC: you need adequate subcutaneous fat at the chosen location.
- For IM: you need sufficient muscle thickness and correct landmarking.
3) Reduce repeat-dose friction
B12 injections are often repeated (weekly, biweekly, or monthly depending on the regimen). In my experience, the single biggest quality-of-life improvement comes from a simple, consistent rotation plan—so people don’t use the same tender spot every time.
4) Use a rotation schedule, not random “trial-and-error”
Random site selection increases the odds you’ll hit scar tissue, inflamed areas, or unusually sensitive spots. Rotating within the recommended injection site region supports better tolerance.
Technique Snapshot: What Most People Get Wrong
I’ll keep this practical and grounded in what I’ve seen repeatedly:
- Poor landmarking: especially relevant for IM buttock injections. If landmarks aren’t clear, discomfort and avoidable issues increase.
- Inconsistent angle/depth: route matters (IM vs SC), and so does needle selection/approach.
- No site rotation: repeated injections into the same place can cause thicker localized tissue and more pain.
- Skipping prep: poor cleaning habits can increase irritation even when the medication itself is fine.
Even when people know the “right” injection site, inconsistency in technique is where outcomes vary. The best way to give b12 injection is the method you can repeat correctly every time.
Injection Site Rotation: A Simple, Repeatable Plan
If you’re doing multiple doses, rotation helps keep local tissue calm. Here’s a straightforward approach I recommend in caregiver training sessions:
For IM dosing
- Pick one IM site region that’s easiest to access consistently (commonly thigh) and rotate within that region (e.g., slightly different spots day-to-day).
- Leave tender areas alone for the next cycle.
- Keep a simple log (date + site) so you can spot patterns in soreness.
For SC dosing
- Rotate between abdomen, thigh, and/or upper arm as allowed by your regimen and anatomy.
- Use a consistent “path” across the abdomen or thigh to avoid repeatedly striking the same area.
- Avoid injection into areas with irritation, redness, or lumps.
What I’ve observed: people who track site choice for just 2–4 weeks often stop guessing, which reduces both anxiety and repeat-injection errors.
When to Get Help (Practical Red Flags)
Most injection discomfort is minor and short-lived, but it’s smart to know when to seek guidance. Contact a clinician promptly if you notice:
- Severe or worsening pain
- Large swelling, redness that spreads, or warmth at the injection site
- Signs of infection (increasing tenderness, fever)
- Unusual reactions such as persistent rash or breathing difficulty
- Repeated difficulty locating landmarks or consistent injection trauma
In my experience, the earlier you adjust technique with professional input, the faster comfort improves—especially for self-injectors.
FAQ
What is the best way to give b12 injection for most people: IM or SC?
The best way depends on the prescribed route for your specific B12 formulation. IM and SC can both be used in different regimens; the correct injection sites follow the route your clinician ordered.
Where should I inject vitamin B12 if I’m self-administering?
Many people find the outer thigh convenient for IM dosing and easier to learn. For SC dosing, abdomen (avoiding the immediate navel area), thigh, or upper arm can work well if there’s enough subcutaneous tissue.
How often should I rotate vitamin B12 injection sites?
Rotate with every dose when the regimen is repeated. Aim to use a new spot within the recommended site region and avoid areas that are still tender or inflamed.
Conclusion: Your Next Practical Step
Vitamin B12 injection sites aren’t a minor detail—they directly affect comfort, consistency, and the reliability of your routine. The best way to give b12 injection is to match the site to the prescribed route (IM vs SC), use clear landmarks or accessible regions (often the thigh), and rotate systematically across doses to minimize irritation.
Next step: write down your prescribed route (IM or SC) and choose one primary site region you can access consistently, then create a simple rotation plan for your next 2–4 doses.
Discussion