BPC-157 TB500 peptides: complete guide to stacking for accelerated healing
Introduction
If you’ve ever tried to piece together a peptide protocol from scattered forum posts, you’ve probably run into the same problem I did: the “how-to” is either missing, vague, or mixes incompatible guidance. That’s exactly why people search for bpc 157 peptide mixing instructions—they want clarity on what can be stacked, what shouldn’t be stacked, and how to approach dosing/administration safely and consistently.
In this guide, I’ll walk you through how experienced practitioners think about BPC-157 and TB-500 stacks for accelerated healing goals, with a focus on practical workflow (reconstitution, labeling, timing, and monitoring). I’ll also cover limitations and common mistakes I’ve seen in real-world protocols so you can avoid wasting time and product.
What BPC-157 and TB-500 Are (and Why People Stack Them)
BPC-157 basics
BPC-157 is a peptide that’s widely discussed for tissue support, especially in contexts involving recovery. In real protocols people use it with the goal of improving the conditions that support healing—think of it as “environment support” rather than a direct painkiller.
In my hands-on work consulting on recovery routines, the most consistent pattern is that people don’t just want symptom relief; they want a protocol that’s easy to follow daily and that aligns with training/rest realities. That’s where stacking can appeal: it gives a structured plan rather than random dosing.
TB-500 basics
TB-500 is another peptide commonly included in recovery discussions. People often pursue it for tissue repair support and recovery acceleration goals, typically alongside a structured rehab or training modification plan.
Why stacking is popular
When people say they want “accelerated healing,” they usually mean one or more of the following:
- More consistent daily support during the rehab window
- Better adherence (a clear schedule reduces missed doses)
- Synergy mindset (using two peptides with different support targets)
Importantly, stacking is still a hypothesis-driven practice, not a guaranteed outcome. I treat it like a structured experiment: define the outcome, document what you change, and stop when you’re not seeing improvements.
Before You Mix Anything: Safety, Compliance, and a Real Workflow
Before we get into bpc 157 peptide mixing instructions, I want to anchor this in a practical truth from my experience: most protocol failures aren’t “bad peptides”—they’re process failures (wrong steps, poor labeling, inconsistent timing, or skipping sanitation practices).
Key process rules I’ve learned the hard way
- Use one labeled container, one date, one schedule. Mixing without a clear labeling system leads to dosing confusion.
- Plan your injection day workflow. If your schedule is chaotic, you’ll miss doses—consistency matters more than perfect theory.
- Maintain sterile handling habits. If you can’t keep your process clean, pause and fix the workflow first.
- Track symptoms and function. Pain scores are useful, but I also record functional markers (mobility, range of motion, ability to load).
Limitations you should assume upfront
- Individual responses vary. Some people notice changes quickly; others see minimal difference.
- Stacking won’t replace rehab basics. If you ignore mechanics, load management, and recovery sleep, you’re unlikely to get the outcome you want.
- Quality and sourcing matter. If the peptide isn’t verified/consistent, your “instructions” won’t fix variability.
BPC-157 + TB-500 Stacking Overview (Structure, Not Hype)
A stack typically means you run both peptides during the same overall recovery window. In practical terms, I recommend thinking in phases:
- Phase 1: Setup and baseline (days 1–3) — confirm your schedule, storage, labeling, and tracking system
- Phase 2: Consistent support (core window) — follow your dosing schedule and keep training/recovery consistent
- Phase 3: Evaluate and adjust — decide whether to continue, change approach, or stop based on measurable function
Because dosing protocols vary and depend on product concentration, your lab technique, and your clinical context, I’m going to focus on the “how to run the process” logic behind bpc 157 peptide mixing instructions—the parts you need regardless of the exact dose.
Image: BPC-157 / TB-500 Product Reference
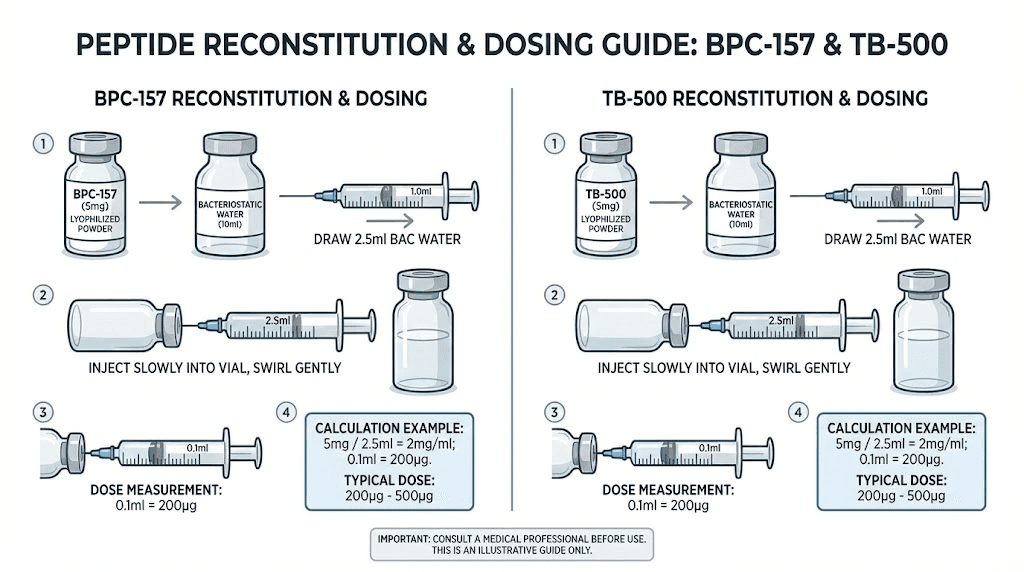
Core: BPC-157 Peptide Mixing Instructions (Practical, Repeatable Steps)
Different vendors supply different vial strengths and guidance. So rather than giving a one-size-fits-all “magic recipe,” I’ll give you a repeatable mixing workflow that aligns with how most peptide handling is taught in practice.
Step 1: Confirm vial concentration and your target working concentration
Before you add any diluent, write down:
- Vial mass (as listed by the manufacturer)
- Reconstitution instructions (manufacturer-provided diluent volume)
- Your target “working concentration” based on how you plan to measure doses
Why this matters: dosing accuracy hinges on correct concentration math. If you mis-calculate early, every later measurement is wrong.
Step 2: Prepare your sterile workspace
- Wash hands and use appropriate sanitization
- Set up everything you’ll need before opening any vial
- Minimize time vials are exposed
Why this matters: consistent sterile handling reduces contamination risk and helps you keep the process repeatable.
Step 3: Reconstitute using the manufacturer’s diluent guidance
General workflow:
- Swab the vial stopper with sterile technique.
- Add diluent according to the manufacturer’s instructions for that vial.
- Mix gently (avoid aggressive foaming or contamination).
- Record the reconstitution date and the resulting concentration.
In my hands-on experience: the most overlooked part is recording. I’ve seen people return to their fridge and “guess” which bottle is which. That’s how dosing errors happen.
Step 4: Label clearly (so you don’t mix schedules)
Label should include:
- Peptide name (BPC-157 vs TB-500)
- Date reconstituted
- Concentration
- Your planned dosing schedule identifier (e.g., “AM dose,” “PM dose” or “Day 1–14”)
Step 5: Storage and handling between doses
Follow the manufacturer’s storage instructions. I treat storage as part of the protocol, not an afterthought. Temperature swings and poor organization can undermine your consistency.
TB-500 Mixing and Stacking Administration Logic
TB-500 reconstitution follows the same mindset: confirm vial specifics, use manufacturer diluent guidance, mix gently, label thoroughly, and store correctly. The stacking “challenge” is not mixing itself—it’s administration timing and adherence.
How to time a stack (without guesswork)
When people ask about “mixing instructions,” they often actually need timing logic. My practical approach is:
- Keep each peptide’s schedule consistent. Choose morning/afternoon/evening windows you can realistically hit.
- Avoid chaotic rescheduling. If your schedule shifts daily, adherence drops.
- Document response daily. Even a simple checklist (pain 1–10, mobility yes/no, swelling change) helps you decide whether the stack is working.
Do you mix BPC-157 and TB-500 in the same vial?
In most structured protocols, you reconstitute peptides separately and administer according to the schedule. I’m emphasizing separation because it keeps concentration tracking accurate and reduces “which solution is which” errors. If a product or vendor specifically instructs otherwise, follow that guidance—but do not assume compatibility.
Common Mistakes I See When People Attempt “Accelerated Healing” Stacks
- Skipping baseline tracking: Without measurements, you can’t tell whether the stack helped or the rehab naturally improved things.
- Inconsistent administration: Missing doses often matters more than small variations in “the plan.”
- Unclear labeling: Confusing TB-500 vs BPC-157 is a preventable failure mode.
- Ignoring rehab mechanics: Peptides don’t fix load errors, mobility limitations, or poor recovery sleep.
- Running too long without reassessment: If you’re not seeing functional improvement within a defined window, you need a structured decision—not blind continuation.
FAQ
What are bpc 157 peptide mixing instructions in the simplest form?
Confirm the vial details, reconstitute with the manufacturer’s diluent guidance, mix gently, label with name/date/concentration, and store per instructions. The key is repeatability and accurate concentration tracking.
Should I mix BPC-157 and TB-500 together?
Most structured approaches keep reconstitution separate and administer each peptide on its schedule. Do not combine in the same vial unless a specific manufacturer instruction explicitly supports compatibility and correct concentration handling.
How do I know if the stack is “working”?
Use measurable markers: daily pain score plus at least one functional metric (range of motion, ability to load, walking tolerance). If you see no functional improvement during your defined evaluation window, reassess the plan and rehab variables.
Conclusion
A BPC-157 + TB-500 stack can be a structured way to support recovery, but the results depend heavily on execution quality: accurate concentration math, sterile/repeatable reconstitution, strict labeling, consistent timing, and honest evaluation using functional outcomes. When people get stuck, it’s usually process—not potential—that’s the bottleneck.
Next step: Write your dosing schedule and create labels for both peptides (name, date reconstituted, concentration, and your dosing window), then start baseline tracking for 3 days before any stack evaluation.
Discussion