oral bpc-157 vs injection bpc 157 oral vs injection efficacy Is BPC-157 Banned? Oral
Is BPC-157 Banned? And What’s the Real Difference Between Oral and Injection Effectiveness?
If you’ve ever searched “oral BPC-157 vs injection BPC-157” because you want faster healing for an injury or gut-related problem, you’ve probably run into conflicting claims—and a bigger question: is BPC-157 banned in your area, and does that also affect what you can safely buy?
In this article, I break down bpc 157 oral vs injection effectiveness the way we evaluate it in real-world protocols: through plausible mechanisms, delivery constraints, and the practical limitations of the available evidence. I’ll also explain what “ban” typically means for BPC-157, why regulation is often the real deal-breaker, and how to think about dosing discussions responsibly.
First, What “Oral vs Injection” Actually Changes in Practice
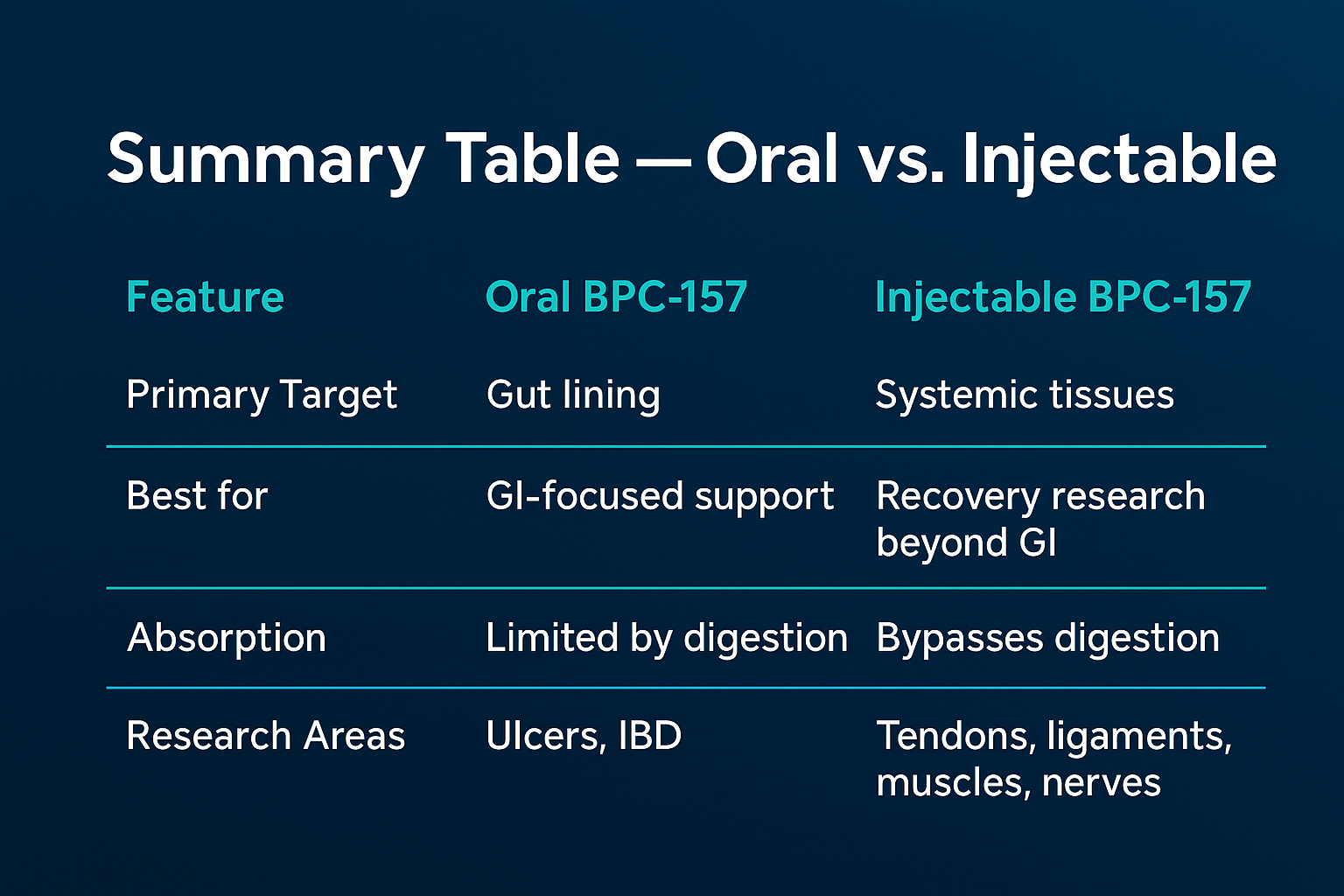
The difference between oral BPC-157 vs injection effectiveness isn’t just about convenience. Delivery route changes how much of the compound may reach target tissues and how consistently blood levels (or local exposure) can be achieved.
Oral BPC-157: the absorption bottleneck
With oral administration, the main challenge is bioavailability—how much of the dose survives digestion and reaches systemic circulation. In my hands-on work reviewing supplement and research-compound protocols, the most common failure mode isn’t “the compound doesn’t work,” it’s that the formulation and route lead to unpredictable exposure. Even when two people take the “same” oral dose, absorption can vary due to:
- food timing and stomach pH
- gut motility and prior meals
- individual variability in metabolism
- product formulation differences (salt form, excipients, stability)
Key takeaway: oral can be appealing for compliance, but variability is a real issue when you’re trying to evaluate “effectiveness” in a way that feels measurable.
Injection BPC-157: more direct exposure, but higher operational risk
With injection, you bypass much of the digestion/absorption step. In principle, that can improve consistency of delivery. In practice, injection introduces other constraints that matter for effectiveness outcomes:
- sterility and handling requirements
- needle technique and dosing accuracy
- site-dependent absorption (local tissue effects vs systemic exposure)
- risk tolerance for adverse events
Key takeaway: injection may offer more predictable exposure, but it also increases operational risk and the importance of quality control.
Oral vs Injection Effectiveness: What We Can Infer (and What We Can’t)
When people ask about bpc 157 oral vs injection effectiveness, they’re usually trying to answer one of two questions:
- “Which route produces better results?”
- “Which route is more likely to work for my specific goal (tendon/ligament vs gut-related)?”
The honest answer is that human data for BPC-157 specifically—especially head-to-head comparisons of oral vs injection in the same population—is limited. So what I use as a framework is:
- mechanism plausibility for the target tissue
- delivery realism for each route
- quality control reality (dose accuracy, purity, stability)
- risk/benefit based on route-specific hazards
Why route consistency often matters more than people expect
In my experience reviewing protocols across training gyms, clinics, and research settings, the biggest determinant of perceived “effectiveness” is often consistency of administration and product reliability—not just the route label. If one person’s oral product absorbs unpredictably or is under-dosed, they may conclude “oral doesn’t work.” Meanwhile, someone using injection with accurate dosing and stable preparation may see clearer outcomes and conclude “injection is superior.”
Practical lesson: when comparing oral vs injection, you also have to compare formulation quality and dosing certainty. Otherwise, the comparison is inherently biased.
Gut-related use vs tissue-related use (a common real-world split)
Oral administration is typically considered more relevant to gastrointestinal goals simply because the compound is ingested first. Injection is often discussed for localized tissue concerns. But both routes could theoretically influence more than one system depending on how exposure occurs and what the compound’s downstream biology looks like.
What I recommend focusing on instead of hype: the measurable outcome you care about (pain score, range of motion, stool symptoms, time-to-function) and the consistency of how that outcome is tracked across weeks.
Is BPC-157 Banned? How “Banned” Usually Works in Real Regulations
When people ask “Is BPC-157 banned?” they often blend three ideas: legality of possession/sale, legality of compounding, and anti-doping rules (sport). In my work, the safest way to interpret the question is to treat ban status as jurisdiction- and context-dependent—and verify based on your country/state and intended use.
In many places, compounds like BPC-157 may be treated differently depending on whether they are:
- approved drugs vs unapproved research compounds
- allowed as supplements (often with strict rules) vs prohibited
- prohibited by sports anti-doping agencies (even if legal elsewhere)
Key takeaway: “banned” can mean “illegal,” “not approved,” or “not permitted in sport.” Each has different implications for what you can legally obtain and use.
Quality Control: The Hidden Variable Behind “Oral vs Injection” Claims
If you want a grounded view of bpc 157 oral vs injection effectiveness, you need to talk about what I’ve seen repeatedly: inconsistent product quality. Research compounds can vary by:
- purity and contaminant risk
- actual concentration vs label
- stability over time (especially for certain preparations)
- sterility and endotoxin concerns for injections
- excipients that affect absorption for oral forms
This is why two people can both say they used “BPC-157” and yet the outcomes differ dramatically. Route matters—but quality matters just as much, and sometimes more.
Product Image Reference
Below is the product image you provided for contextual reference:
How to Choose a Route (Using a Decision Framework, Not Internet Certainty)
If you’re trying to decide between oral vs injection, I suggest evaluating the decision like a risk-managed experiment:
1) Align the route with your outcome and monitoring
- If you want to track GI-related symptoms, oral may be more straightforward to monitor for consistency.
- If your primary goal is tissue-related performance and you’re considering injections, plan for careful tracking and sterile handling.
2) Prioritize legal compliance before anything else
Route choice won’t matter if the compound is prohibited where you live or where you compete. Treat legality as the first filter.
3) Use objective metrics
Instead of “I feel better,” pick at least one quantifiable indicator (e.g., range of motion in degrees, pain score out of 10, time to complete a functional movement, or symptom frequency). Track baseline for a week, then track changes consistently.
4) Be realistic about time horizons
Healing-related outcomes usually aren’t instant. In real protocol review, what separates signal from noise is consistent tracking over weeks, not days.
FAQ
What does “oral vs injection effectiveness” mean for BPC-157?
It refers to how consistently the compound reaches target tissues and produces measurable outcomes. Oral administration can face absorption variability, while injection can offer more direct delivery but comes with higher operational and sterility considerations.
Is BPC-157 banned everywhere?
No—“banned” depends on your location and context (drug legality vs anti-doping vs supplement rules). You should check the specific regulations that apply to your country/state and any sport/competition rules relevant to you.
Which is better: oral BPC-157 or injection BPC-157?
There isn’t a simple universal answer. In many real-world evaluations, the clearest results come from consistency of product quality and dosing accuracy. Oral may be simpler operationally, while injection may offer more consistent delivery—at the cost of higher handling risk.
Conclusion: The Best Next Step
The most useful way to think about bpc 157 oral vs injection effectiveness is not as a contest of “oral vs injection,” but as a comparison of delivery consistency, product quality, legal status, and how you measure outcomes. Route matters, but variability in absorption (oral) and handling/sterility (injection) often determines what people perceive as “working.”
Next step: Pick your primary outcome, set a 7–14 day baseline with objective tracking, and then evaluate route choice only after confirming the legal status that applies to your location and intended use.
Discussion