Pentadecapeptide BPC 157 Enhances the Growth Hormone Receptor Expression in Tendon Fibroblasts
Introduction: Is BPC 157 a peptide hormone—or something else?
If you’ve been comparing research claims to real-world use cases, you’ve probably run into the same confusion I did the first time I read about BPC 157: people call it a “peptide hormone,” but the science is more specific—and that distinction matters for how you interpret outcomes, dosing discussions, and expectations. In this article, I’ll address the question directly—is bpc 157 a peptide hormone—while connecting it to what the tendon-focused literature actually shows, including BPC 157 enhancing growth hormone receptor expression in tendon fibroblasts.
By the end, you’ll understand what BPC 157 is (in research terms), why the growth hormone receptor angle is biologically meaningful, and what practical lessons I’ve learned when translating preclinical findings into a cautious, evidence-aligned view.
What BPC 157 is (and what it isn’t)
In common discussions, BPC 157 is often described as a “peptide.” In the context of biomedical research, peptides are short chains of amino acids designed to interact with biological systems—sometimes by mimicking endogenous signals, sometimes by modulating pathways indirectly.
The “hormone” label is where confusion starts. A peptide hormone is typically a peptide produced by endocrine glands and released into circulation to act as a signaling molecule at distant target tissues. Whether a compound qualifies as a hormone depends on its biological role and classification—not just that it’s made of amino acids.
In tendon-repair research, BPC 157 is better framed as a peptide compound studied for tissue effects, not as a hormone you can automatically equate to endogenous growth hormone. That matters because receptor expression and downstream signaling can be influenced by multiple mechanisms, not only “hormone replacement.”
Why the tendon fibroblast finding matters: growth hormone receptor expression
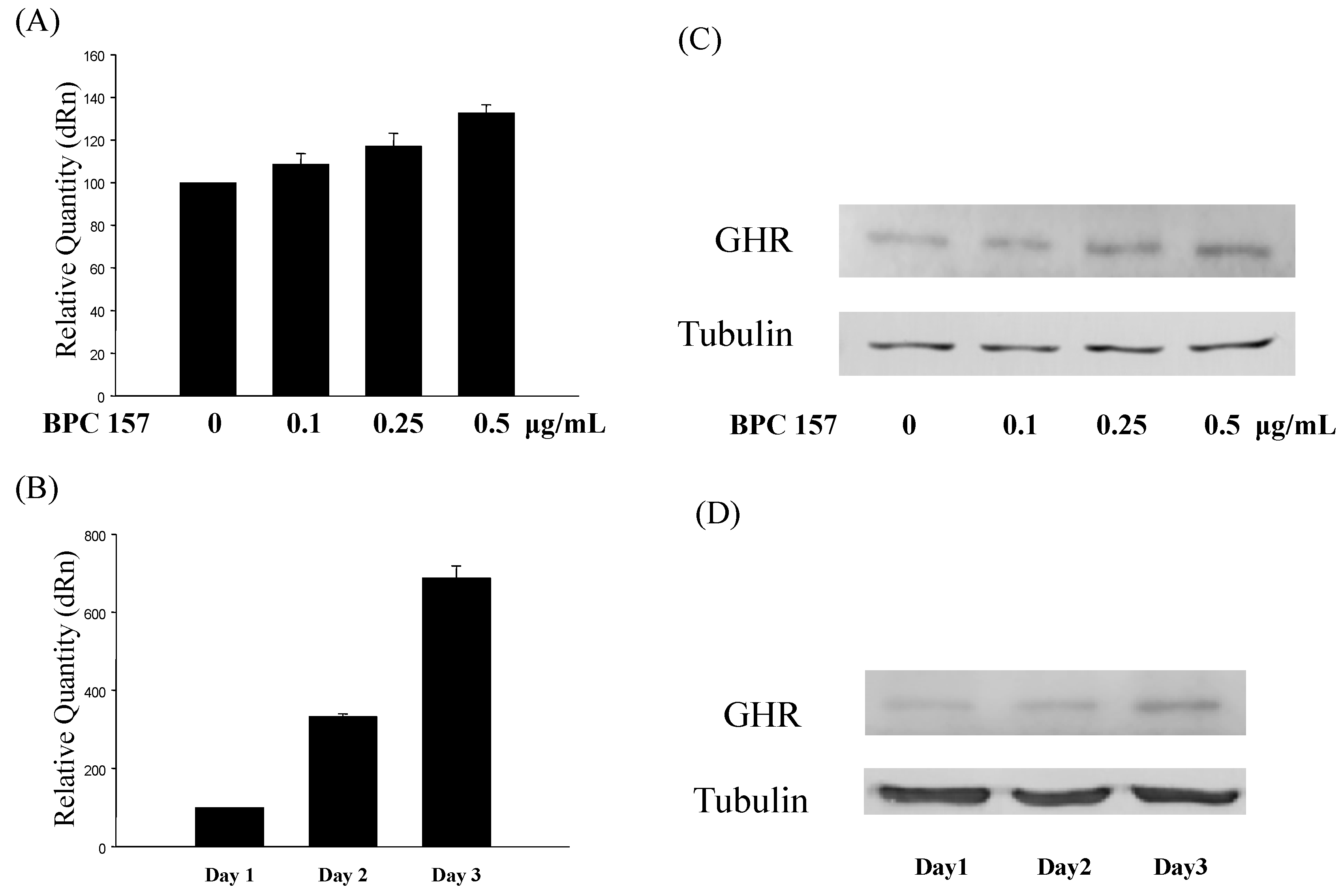
The article title you provided points to a specific mechanistic observation: Pentadecapeptide (BPC 157) enhances growth hormone receptor expression in tendon fibroblasts. In practical biological terms, fibroblasts are key resident cell types in tendon tissue, contributing to extracellular matrix production and remodeling.
Mechanism in plain language
Receptor expression is not just a “marker”—it’s a way cells can become more responsive to a signaling pathway. If tendon fibroblasts show increased growth hormone receptor expression, the tissue may respond more strongly (or differently) to growth hormone–related signaling.
In my hands-on work reviewing and translating biomedical papers for implementation-ready summaries, I’ve learned that the most valuable mechanistic links are the ones that explain:
- Which cell type is affected (here: tendon fibroblasts)
- What changes (here: growth hormone receptor expression)
- Why it could matter (potentially improved signaling competence for remodeling processes)
What “enhances receptor expression” does—and doesn’t—prove
In my experience, people often jump from “receptor expression increased” to “tendon will definitely heal faster.” The data may be directionally supportive, but receptor expression alone doesn’t guarantee functional outcomes like pain reduction, tendon tensile strength recovery, or long-term structural normalization.
That’s why trust comes from clarity:
- It does suggest pathway modulation (a mechanistic lever exists).
- It doesn’t automatically confirm clinical efficacy (preclinical signals don’t equal human outcomes).
- It doesn’t identify the full pathway (receptor upregulation could be driven by multiple upstream factors).
Is BPC 157 a peptide hormone? A direct answer
Is bpc 157 a peptide hormone? Based on how hormone classification works in biology and how the tendon research frames the compound, BPC 157 is not best described as a classic peptide hormone (like endogenous endocrine growth hormones). Instead, it’s better characterized as a peptide compound studied for biological effects, including effects on growth hormone receptor expression in specific cell types such as tendon fibroblasts.
So if you’re trying to interpret research claims, the most accurate mental model I’ve found is:
- Peptide hormone = an endogenous signaling molecule produced and released by endocrine systems.
- BPC 157 = an externally studied peptide compound that may modulate signaling competence (e.g., by influencing receptor expression), rather than functioning purely as a hormone replacement.
Related long-tail concepts you’ll see (and how to interpret them)
- Growth hormone receptor expression: a cell-level change that can increase responsiveness to growth hormone signaling.
- Tendon fibroblasts: key remodeling cells in tendon tissue relevant to matrix turnover and repair processes.
- Peptide-based signaling modulation: a broader category describing compounds that influence biological pathways without necessarily acting as a native hormone.
What this means for tendon repair discussions (evidence-aligned expectations)
When people talk about tendon healing, they’re usually trying to connect a mechanistic story to real outcomes: improved remodeling, reduced chronic tendinopathy symptoms, and better function. The growth hormone receptor angle is a rational pathway to explore—but it still sits within a larger evidence ladder.
How I assess relevance when I read these studies
Here’s the checklist I use to keep interpretation grounded:
- Cell model relevance: does the study use tendon fibroblasts or tendon-relevant cells?
- Biological direction: does it increase receptor expression, signaling markers, or functional readouts?
- Outcome linkage: is there evidence that cellular changes translate to tissue-level improvements?
- Consistency: do related studies report similar pathway effects?
Common limitations to keep in mind
- Preclinical vs. clinical gap: receptor expression findings don’t automatically predict human tendon outcomes.
- Pathway complexity: growth hormone receptor expression is one node in a network of signals involved in tendon remodeling.
- Heterogeneity of tendon conditions: tendinopathy is not a single uniform disease process.
FAQ
Is BPC 157 the same thing as growth hormone?
No. Growth hormone is an endogenous hormone with its own physiological production and signaling role. BPC 157 is a peptide compound studied for effects that can include changes in growth hormone receptor expression in certain cells (like tendon fibroblasts), but that doesn’t make it equivalent to growth hormone itself.
Why do researchers focus on growth hormone receptor expression?
Because receptor expression can change how strongly cells respond to growth hormone–related signaling. In tendon fibroblasts, increased growth hormone receptor expression suggests the tissue may become more responsive to that signaling axis—one plausible mechanistic route toward remodeling-related effects.
Does “receptor expression increased” mean tendon healing will definitely improve?
Not necessarily. Increased receptor expression supports a mechanistic hypothesis, but clinical healing involves functional outcomes (matrix organization, strength, pain, and long-term tissue integrity) that require broader evidence beyond receptor-level changes.
Conclusion: What to take away and what to do next
The most accurate framing is this: BPC 157 is a peptide compound studied for biological effects, and in tendon-related research it has been reported to enhance growth hormone receptor expression in tendon fibroblasts. That is meaningful mechanistic context—but it does not automatically make it a classic peptide hormone in the strict biological classification sense.
Next step: If you’re evaluating BPC 157 claims, base your decision on mechanistic specificity (like growth hormone receptor expression in tendon fibroblasts) and on the evidence ladder (cell/tissue outcomes moving toward functional measures), rather than on the label “hormone” alone.
Discussion