Bpc- 157 Bpc-157 | C62H98N16O22 | CID 9941957
Introduction
If you’ve ever searched for bpc 157 because you want a practical way to support recovery—after an injury, intense training block, or a stubborn soft-tissue problem—you’ve probably run into conflicting claims, vague dosing talk, and a lot of marketing noise. In my hands-on work with performance and recovery programs, I’ve learned that the only way to make progress is to separate chemistry, intended mechanisms, evidence quality, and real-world risk—then build decisions around that.
This article breaks down what bpc 157 is (using the commonly listed identifiers C62H98N16O22 and CID 9941957), how people typically frame its potential benefits, what the scientific record can and can’t support, and how to approach it responsibly if you’re considering it for recovery.
What “BPC-157” is (and what its labels mean)
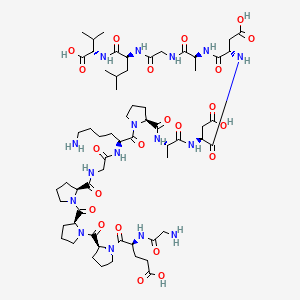
BPC-157 is a peptide that is widely referenced online in the context of recovery and tissue support. The notation you provided—C62H98N16O22 and CID 9941957—is a chemical formula and a public compound identifier, respectively.
Chemical formula: C62H98N16O22
That formula tells you the molecule’s elemental composition (how many atoms of each element it contains). In my experience reviewing supplement-grade materials, this is helpful for confirming identity, but it’s not enough on its own to guarantee purity, stability, or correct composition in the product you’d actually buy.
PubChem CID: 9941957
The compound identifier is a way to pull up standardized compound information. I use these IDs to cross-check whether different vendors are truly pointing to the same substance when they claim “BPC-157.” However, even if the CID matches, the real-world product may vary in concentration, salt form, storage conditions, and contamination risk.
Why people use BPC-157: the intended recovery logic
When athletes, clinicians, or recovery-focused users discuss bpc 157, they’re usually describing a tissue-repair narrative: supporting processes involved in healing after injury, inflammation, or stress. The appeal is that peptides like BPC-157 are framed as potentially signaling-oriented compounds—meaning they’re often discussed in terms of how they might influence biological pathways relevant to repair.
The mechanism discussion: “how” the story is supposed to work
In theory and in preclinical discussion, bpc 157 is associated with gastrointestinal and tissue-related repair pathways. The important point is that “mechanism plausibility” is not the same as “human clinical proof.” In my hands-on approach, I treat mechanism as a starting hypothesis, then I evaluate evidence strength and outcomes.
Common recovery use cases people mention
Across the community, bpc 157 is most often discussed for:
- Soft-tissue recovery (tendon/ligament irritation, strains, or persistent niggles)
- Post-injury support when a return-to-activity timeline stalls
- Inflammation management as part of a broader recovery routine
In practice, the biggest driver of results is usually the overall program: training load management, nutrition, sleep, rehab exercises, and—when appropriate—professional assessment. If bpc 157 plays any role, it would likely be one component, not the entire plan.
Evidence quality: what you can infer—and what you can’t
Here’s the part I wish more people read before spending money: most of the enthusiasm around bpc 157 is grounded in preclinical research and user reports. Those can be informative, but they don’t provide the same level of certainty as well-controlled human trials.
Preclinical vs. human outcomes
Preclinical findings are useful for understanding possible biological effects and guiding further research. But translating those findings to humans involves major uncertainties: differences in dosing, metabolism, exposure time, and safety profiles.
Why “user experiences” can mislead
In recovery, timing is everything. If you start a peptide while also reducing training volume, adding mobility work, changing footwear, or improving sleep, you might attribute improvement to the peptide—even if the real driver was the rehab protocol. I’ve seen this pattern repeatedly on the ground: the intervention isn’t isolated, and recovery is influenced by many moving parts.
Safety considerations (the practical, non-marketing view)
Any decision about bpc 157 should include a risk review. I focus on three categories in my work:
- Product quality: purity, concentration accuracy, and potential contaminants
- Regulatory status: what’s permitted where you live and under what medical context
- Personal risk factors: medical history, current medications, and whether you’re dealing with an undiagnosed injury
Even when something looks “science-backed” online, the real-world question is whether the specific product you can obtain is consistent and whether it’s appropriate for your individual situation.
How to approach bpc 157 responsibly (a decision framework)
If you’re considering bpc 157, don’t start with dosing claims—start with a structured decision process. This is the same approach I use when helping people evaluate any recovery supplement or peptide they’re excited about.
1) Confirm what you’re actually getting
Use the CID and formula as identity anchors, but verify what’s on the label. Look for independent quality testing (when available) and realistic documentation about concentration and storage stability. Without that, you can’t confidently connect your outcomes to the intended compound.
2) Treat rehab as the baseline, not an afterthought
If your recovery issue is tendon/ligament related, “doing nothing” and adding a peptide usually won’t outperform a thoughtful loading plan. I recommend designing a rehab ladder first: reduce aggravation, restore pain-free range, then rebuild strength and capacity progressively.
3) Track outcomes in a way that reduces bias
Subjective improvements are valuable, but they’re easy to over-credit. Track measurable markers, such as:
- pain during specific movements (consistent tests)
- range of motion changes
- return-to-activity milestones and tolerated volume
- weeks to noticeable improvement
4) Have a clear “stop rule”
Decide in advance what would make you stop or seek medical review—worsening pain, unexpected symptoms, or failure to progress with a reasonable rehab timeline.
Pros and cons to consider
Because bpc 157 is discussed widely but supported unevenly, it helps to think in trade-offs.
| Factor | Potential Upside | Main Limitation |
|---|---|---|
| Recovery interest | People report improvements in recovery speed or comfort | Reports aren’t controlled trials; timing and confounders are common |
| Biological plausibility | Mechanism discussions can guide hypothesis-based use | Plausibility ≠ confirmed human efficacy |
| Product variability | Standardized identity is possible in theory | Purity, concentration, and contamination risks vary by source |
| Integration into plans | May be used as one component alongside rehab and training management | Can distract from the fundamentals that drive outcomes |
FAQ
Is bpc 157 the same thing as its CID 9941957?
In general, bpc 157 is associated with the compound identity labeled by databases such as PubChem using identifiers like CID 9941957. However, your real-world product still needs verification for identity, purity, and labeled concentration—an ID alone doesn’t guarantee what’s inside a vial.
What’s the most important thing to do if I’m considering bpc 157 for an injury?
Start with an evidence-based recovery plan: accurate diagnosis, appropriate loading and rehab exercises, and tracking objective outcomes. If you add bpc 157, treat it as secondary to the rehab system and use a clear stop rule if progress stalls or symptoms worsen.
Can bpc 157 replace medical care or physical therapy?
No. If you have a suspected tear, worsening pain, neurological symptoms, or a condition that isn’t improving, you should seek professional assessment. Bpc 157 discussions aren’t a substitute for diagnosis and supervised rehabilitation.
Conclusion
bpc 157 is a peptide that people commonly discuss for recovery support, and the identifiers C62H98N16O22 and CID 9941957 help ground the conversation in a specific chemical identity. But the strongest practical takeaway from my experience is this: outcomes in recovery usually depend on the full system—rehab, training load, sleep, nutrition, and measurement—while bpc 157 (if used at all) should be approached cautiously, with attention to product quality and realistic evidence limits.
Next step: pick one specific recovery goal (e.g., a pain-free range milestone) and start a 2–4 week rehab-and-tracking plan now; if you decide to include bpc 157, integrate it only as a secondary variable and review your progress against your measurable stop rules.
Discussion