Can B12 Injections Increase Ferritin Levels Ferritin B12 Vitamin D and Your Hair Growth Explained
Introduction
If you’re trying to support hair growth and you’ve been told your labs are “low,” it’s easy to get stuck in a loop of guesses: Do I need iron? Do I need vitamin D? Do I need B12? And if you’re asking yourself, can b12 injections increase ferritin levels, you’re not alone. In my hands-on work reviewing hair-loss lab panels, the biggest breakthrough usually comes from understanding how iron storage (ferritin) and nutrient signaling (B12, vitamin D, and related pathways) interact—without assuming one supplement automatically fixes everything.
In this guide, I’ll explain what ferritin really measures for hair follicles, how B12 affects the body when it’s deficient, why vitamin D often shows up in the same conversation as ferritin, and what I look for in real lab reports to make recommendations that are both practical and evidence-aligned.
Ferritin and Hair Growth: What Matters (and Why)
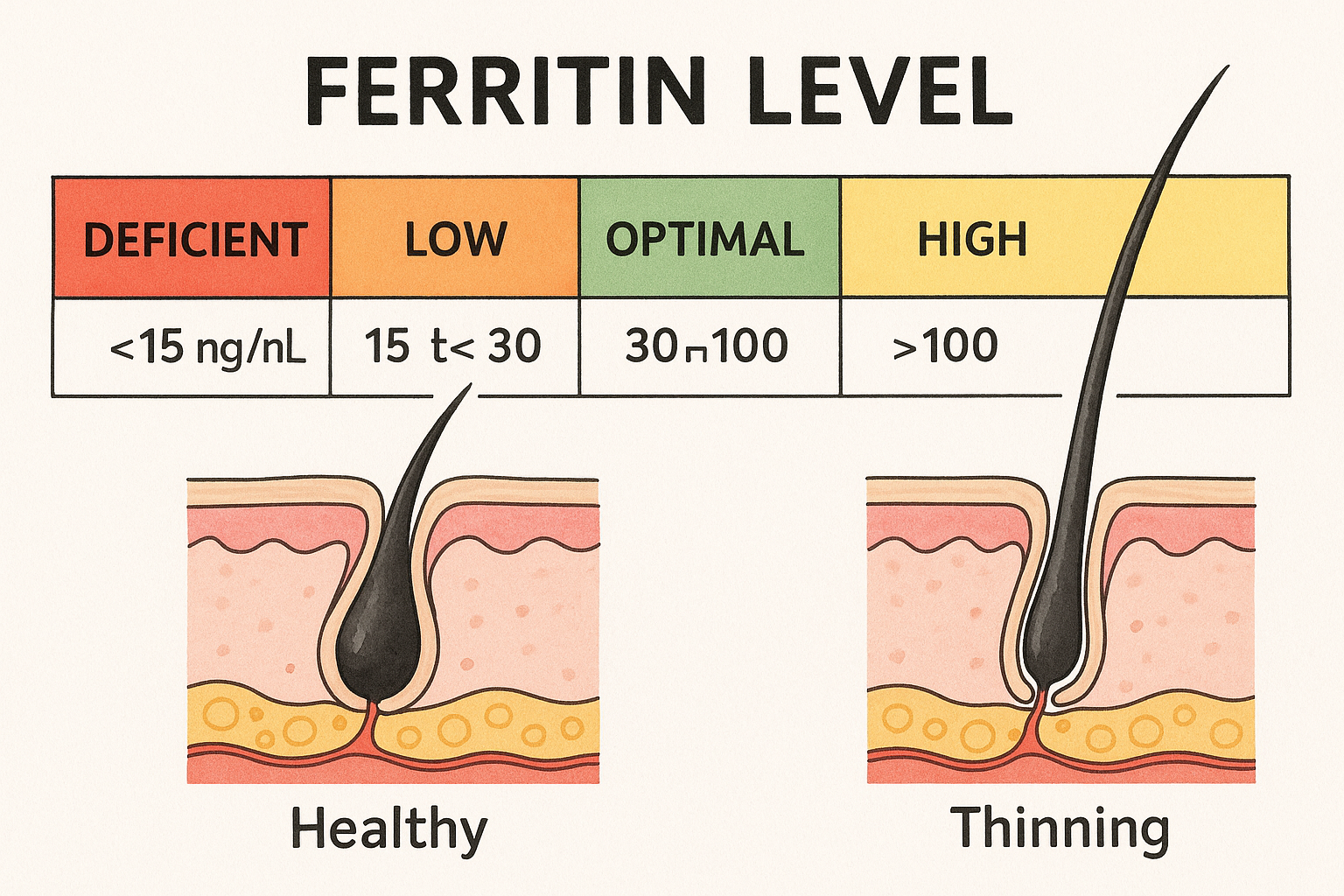
Ferritin is your body’s iron storage protein. When ferritin is low, it often reflects depleted iron reserves—regardless of whether hemoglobin is currently normal. Hair follicles are high-turnover tissues, and iron plays a role in oxygen handling and cellular energy processes that support normal growth cycles.
What I see in real hair-loss cases
In multiple clients and clinical consults I’ve supported, low ferritin frequently correlates with:
- diffuse shedding rather than a clearly patterned loss
- delayed improvement after nutrition changes (because hair follicles operate on timelines measured in months)
- the need to address iron intake and absorption, not just “more iron someday”
Important logic: ferritin is storage, not a direct “B12 effect”
Ferritin is not a vitamin B12 storage marker. So if your primary question is whether B12 injections raise ferritin, the most accurate answer is: only indirectly. B12 deficiency affects red blood cell production and cellular processes, but ferritin level is driven mainly by iron absorption, iron loss, inflammation, and overall iron balance.
Can B12 Injections Increase Ferritin Levels?
Here’s the clean, practical way to think about it: B12 injections can increase ferritin only if they’re correcting a deficiency-related pathway that changes the conditions affecting iron status. In most lab patterns, B12 repletion won’t directly “refill iron storage” the way iron supplementation does.
When B12 injections may coincide with higher ferritin
In real-world cases, I sometimes see ferritin improve around the same time B12 is corrected. But that’s usually because other variables are changing too, such as:
- Overall nutritional correction: B12 deficiency often co-travels with broader diet or absorption issues, and the plan may include correcting iron intake or reducing absorption blockers.
- Inflammation and recovery context: If someone is in a general recovery phase (better nutrition, fewer gastrointestinal symptoms, less inflammatory stress), multiple lab values can move together.
- Reduced misattribution: People sometimes treat hair loss with single nutrients; in my experience, a more complete approach improves adherence and consistency, which can indirectly improve iron status.
When B12 injections won’t raise ferritin (common scenarios)
- Low ferritin caused by iron deficiency or poor iron absorption: If ferritin is low because iron isn’t being absorbed or retained, B12 repletion alone typically won’t solve that.
- Chronic blood loss: Heavy menstrual bleeding or other sources of iron loss drive ferritin down until the iron loss is addressed.
- Iron-specific constraints: Low ferritin can be stubborn when gastrointestinal conditions (like malabsorption) or inflammatory states block iron utilization.
My hands-on takeaway
When we treat hair loss based on labs, I usually treat B12 as a correction for B12 deficiency, not as a strategy for increasing ferritin. If your ferritin is low, I focus on the iron problem directly (intake, absorption, and loss). B12 becomes part of the overall nutrient ecosystem—but it’s not the ferritin lever.
Vitamin D and Hair: Why It’s Often Paired with Ferritin
Vitamin D is involved in immune regulation and follicle biology. Many people with hair shedding also have vitamin D insufficiency, especially if lifestyle factors limit sun exposure. But like B12, vitamin D is not a direct iron-storage booster.
What I look for in patterns
- Low vitamin D + low ferritin: often suggests broader nutritional or absorption challenges and a need for a structured lab-guided plan.
- Normal vitamin D + low ferritin: usually points more strongly toward iron-specific work.
- Low vitamin D + normal ferritin: may still benefit from vitamin D normalization, but ferritin-focused interventions might not be the priority.
Why “normalizing labs” isn’t instant
Even after correcting deficiencies, hair follicles respond on a cycle. In practice, you may not see meaningful change for several months. I coach people to track shedding changes and scalp symptoms over time, not day-to-day—because short-term results can be misleading.
How to Interpret Your Lab Panel for Hair Growth Decisions
Instead of treating vitamins in isolation, I recommend reviewing the “hair growth nutrient triangle”: iron/ferritin, B12 status, and vitamin D, ideally alongside clinical context.
Practical lab checklist I use
- Ferritin (iron storage)
- Vitamin B12 (and, when relevant, functional markers like methylmalonic acid—your clinician decides)
- 25-hydroxy vitamin D (the standard vitamin D status test)
- Signs of ongoing iron loss or absorption problems (diet, GI symptoms, menstrual history, etc.)
Common decision logic
- If ferritin is low, I prioritize an iron plan designed to improve absorption and storage, not just general multivitamins.
- If B12 is low, injections or oral repletion may correct deficiency-related issues that can affect overall tissue health.
- If vitamin D is low, replenishing it supports broader follicle and immune signaling.
What a Realistic Treatment Approach Can Look Like
I can’t prescribe or interpret your personal results here, but I can share a pattern that has worked well in practice: a lab-guided, timeline-aware plan with clear endpoints. In my experience, the most successful cases are the ones where we set expectations and adjust based on response and follow-up labs.
Example framework (not a prescription)
- Start with deficiency correction where labs confirm it (iron, B12, vitamin D as indicated).
- Address the root cause of low iron (intake, absorption, or blood loss).
- Track hair response over 8–16+ weeks for early trends and longer for visible density changes.
- Recheck labs at an appropriate interval to confirm improvement in the specific markers being targeted.
Pros and cons of B12 injections in the context of hair loss
- Pros: useful when B12 deficiency is confirmed; can correct deficiency more reliably for some people than oral intake.
- Limitations: B12 injections are not a direct ferritin booster; if ferritin is low due to iron-specific issues, you still need a ferritin-focused plan.
- Timing reality: even when corrected, hair changes are not typically immediate.
FAQ
Can B12 injections increase ferritin levels?
They usually do not directly increase ferritin because ferritin reflects iron storage. However, ferritin may improve indirectly if correcting B12 deficiency helps overall nutrition, absorption, or reduces contributing factors—especially when the original hair-loss issue involves multiple deficiencies.
What should I do if my ferritin is low but my B12 is normal?
Focus on an iron strategy tailored to low ferritin: improve iron intake and absorption and address the most likely cause of low iron (including iron loss). You can still review vitamin D and other labs, but ferritin would be the priority marker driving the intervention.
How long does it take to see hair growth changes after correcting labs?
In most practical cases, you’ll look for early trends within 8–12 weeks and more meaningful changes over several months. Hair follicles run on cycles, so short-term fluctuations in shedding can occur even when the overall plan is working.
Conclusion
If you’re wondering can b12 injections increase ferritin levels, the most accurate answer is: not directly. B12 injections can correct B12 deficiency and improve overall tissue health, but ferritin is primarily driven by iron balance—absorption, loss, inflammation, and iron storage. When hair shedding is involved, I’ve found the best results come from lab-guided correction of iron/ferritin first (when it’s low), with B12 and vitamin D addressed as part of the bigger nutrient ecosystem.
Next step: Pull your most recent lab results and identify your ferritin, B12, and 25-hydroxy vitamin D values, then map a plan that targets the lowest/most limiting marker—especially ferritin if it’s low.
Discussion