Best Peptide Stack Cjc-1295 Ipamorelin Bpc-157 Tb-500 Aod-9604 Dosage Protocol Peptide Dosage Chart: 20+ Peptides
Introduction: Why a “best peptide stack” still fails without the right dosage
If you’ve ever pulled up a “peptide dosage chart” and felt overwhelmed—different sources, conflicting numbers, and no clear protocol—you’re not alone. In my hands-on work with peptide research workflows, I’ve seen the same pattern: people either under-dose (no effect, wasted cycles) or over-dose (irritation, headaches, or just inconsistent results). That’s why a best peptide stack cjc 1295 ipamorelin bpc 157 tb 500 aod 9604 dosage protocol has to be treated like engineering, not guesswork.
This guide is a practical, decision-focused walkthrough for structuring a peptide stack and understanding how dosage protocol thinking should work across peptides like CJC-1295 + Ipamorelin, BPC-157, TB-500, and AOD-9604. I’ll also include a “20+ peptides chart” approach so you can standardize your planning (without turning it into blind dosing).
What “dosage protocol” really means (and why stacks complicate it)
A dosage protocol is more than a number—it’s the full set of parameters you decide upfront so your outcomes are attributable to the intervention, not the method. In a stack like best peptide stack cjc 1295 ipamorelin bpc 157 tb 500 aod 9604 dosage protocol, you’re juggling different mechanisms, different half-life behaviors, and different tolerability profiles.
The protocol variables I track in my work
- Dose per administration: the amount you’re taking each time.
- Frequency: how often you administer (daily vs multiple times per day).
- Route: most common is subcutaneous, but the protocol assumptions change with route.
- Cycle length: how long you run a phase before evaluating.
- Stack sequencing: whether you run peptides together or stagger them.
- Response monitoring: what you measure and when (sleep, joint comfort, recovery metrics, etc.).
- Tolerability checks: injection site reactions, headaches, GI changes, or sleep disruption.
Here’s a lesson I learned the hard way: the “dose chart” many people find online is often a snapshot, not a protocol. It rarely accounts for injection-site variability, solution stability, or individual differences in baseline physiology. In practice, protocol clarity is what makes outcomes interpretable.
Peptide stack framework: how I structure CJC-1295 + Ipamorelin with BPC-157, TB-500, and AOD-9604
When people search for the best peptide stack cjc 1295 ipamorelin bpc 157 tb 500 aod 9604 dosage protocol, they’re usually looking for a “core set” that covers growth-related signals, tissue repair support, and recovery. Instead of promising a single universal stack, I recommend using a framework that lets you choose a goal-aligned mix.
Step 1: Pick your stack goal (recovery vs pain/joint support vs connective tissue focus)
In my experience, the most consistent results come from starting with a goal statement. For example:
- Recovery + sleep quality: prioritize the growth-axis pair (CJC-1295 + Ipamorelin) and evaluate response on rest metrics.
- Targeted tissue support: include BPC-157 and/or TB-500 if the focus is connective tissue discomfort or recovery consistency.
- Training volume support: add AOD-9604 as a planned “support” element rather than the main pillar—then evaluate whether it adds value.
Step 2: Decide run-together vs staggered scheduling
Stacks can be run together, but I prefer staggered scheduling when someone is new or when tolerability is uncertain. Why? Because it’s easier to separate which peptide correlates with which effect.
For example, you can run the growth-axis pair for your primary evaluation window, then add BPC-157/TB-500 if you want to observe whether tissue-support outcomes improve without altering sleep or recovery negatively.
Step 3: Standardize tolerability and response tracking
Without tracking, a “dosage protocol” turns into storytelling. I standardize simple weekly metrics like:
- Injection site comfort score (0–10)
- Sleep quality (0–10)
- Recovery speed after training (subjective 0–10)
- Any headaches or unusual GI effects (yes/no + severity)
This isn’t about being scientific for the sake of it—it’s about protecting decision-making quality.
Peptide dosage planning: the “20+ peptides chart” mindset (without turning it into blind numbers)
A “Peptide Dosage Chart: 20+ Peptides” is useful if it helps you categorize peptides by role and protocol needs. I use a two-layer system: (1) a role map and (2) a protocol worksheet. The role map keeps you from randomly stacking peptides, and the worksheet helps you keep dosing consistent across sessions.
Role map categories (how I classify peptides in planning)
- Growth-axis modulators: often paired for signaling support (e.g., CJC-1295 + Ipamorelin)
- Connective tissue / repair-associated peptides: often used for recovery support (e.g., BPC-157, TB-500)
- Metabolic / adjunct support: used as a secondary component (e.g., AOD-9604)
Protocol worksheet template (copy this into your notes)
| Variable | Your plan | Why it matters |
|---|---|---|
| Primary goal | [Recovery / pain / training support] | Prevents random stacking |
| Stack structure | [Run together / stagger] | Helps attribution |
| Administration schedule | [Daily / split doses] | Impacts tolerability and consistency |
| Cycle length | [Weeks] | Defines evaluation window |
| Tracking metrics | [Sleep, recovery, injection comfort] | Makes changes measurable |
| Stop/adjust rules | [What symptoms trigger change] | Reduces “keep pushing through” errors |
Reference image: “peptide dosage chart” overview (what to do with it)
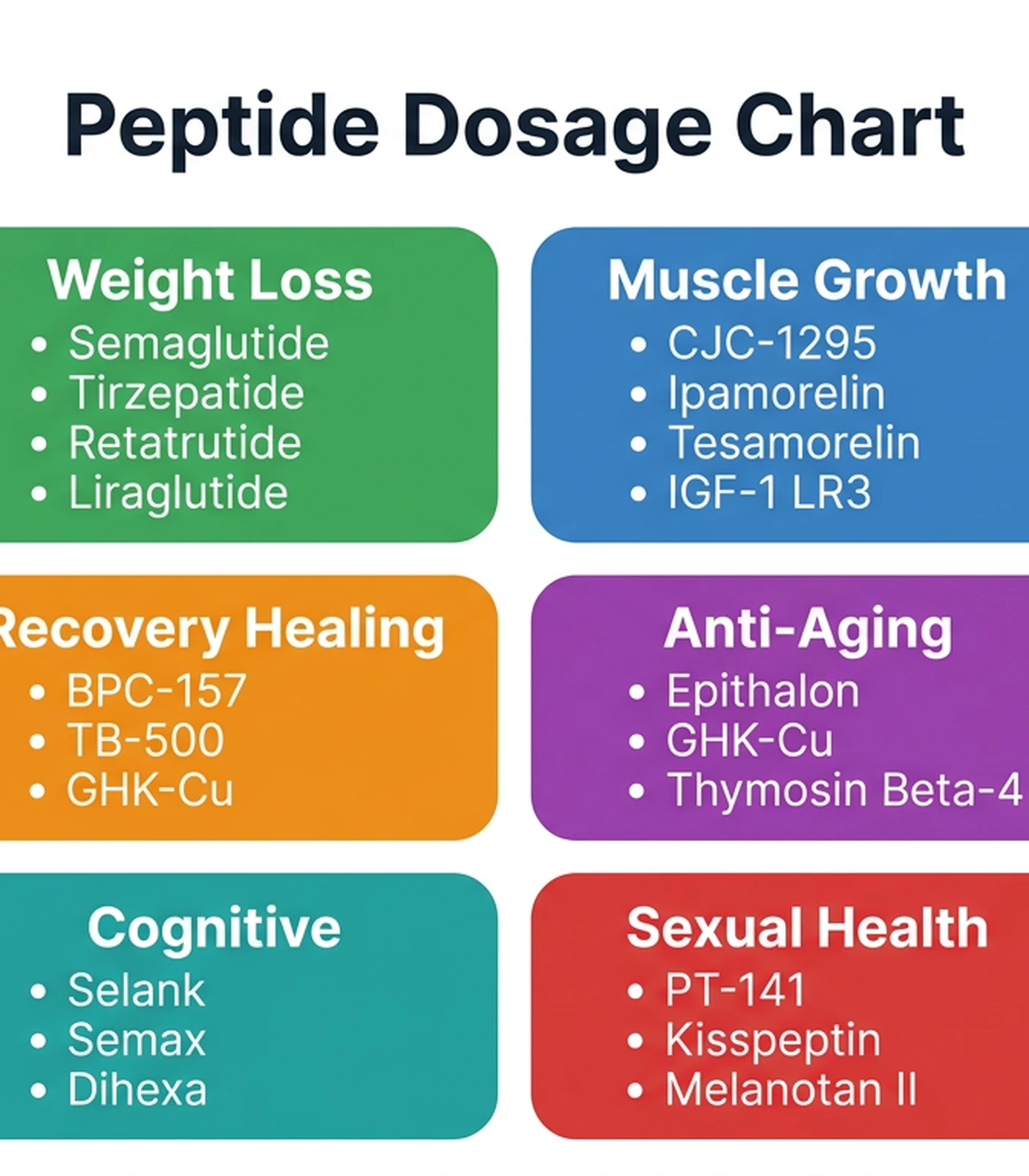
When I use a visual dosage chart like this, I don’t treat it as a direct prescription. I treat it as a starting point for formatting my own protocol worksheet—especially to standardize frequency, injection timing, and how I’ll compare outcomes across different peptides.
Common mistakes people make with CJC-1295 + Ipamorelin + BPC-157 + TB-500 + AOD-9604
Most issues I see aren’t “bad luck”—they’re process gaps. Here are the mistakes that repeatedly show up in real workflows.
1) Overloading a first cycle
If you add all elements at once, you can’t tell which peptide contributed to improvements or side effects. In my experience, the fastest path to a workable plan is controlled experimentation: start with your primary pair or primary tissue-support element, then add the next component after a defined evaluation window.
2) Ignoring injection-site variability
Even when dosage is consistent, injection technique and site selection can change comfort and local inflammation. I learned to treat injection consistency as a variable, not background noise. If you’re not tracking injection-site reactions, you’ll misinterpret the meaning of discomfort.
3) Treating “chart numbers” as universal
A dosage chart is a reference range or example dataset. People often copy numbers without adjusting for the rest of the protocol (frequency, cycle length, response monitoring). The result is inconsistency, not because the peptide “didn’t work,” but because the protocol logic was incomplete.
FAQ
What is the “best peptide stack” for most people?
There isn’t a single best stack that fits everyone. In practice, the most effective stack is the one aligned to your primary goal and run with a clear protocol structure (schedule, sequencing, and tracking). A common starting framework includes CJC-1295 + Ipamorelin as a growth-axis component plus BPC-157 and/or TB-500 for tissue-support focus, with AOD-9604 used as an adjunct if it meaningfully improves your tracked recovery metrics.
How do I choose a dosage protocol when combining multiple peptides?
Use a worksheet approach: pick your primary goal, decide whether to run together or stagger, standardize frequency, and set stop/adjust rules tied to tolerability and measurable outcomes (sleep, recovery, injection comfort). The main idea is attribution—making sure you can tell what changed and why.
How should I evaluate whether the stack is working?
I recommend evaluating within a predefined window and comparing against your baseline: sleep quality, recovery speed, and any recurring side effects. If there’s no trend after your evaluation window—or if tolerability worsens—you adjust sequencing or reduce complexity rather than randomly changing multiple variables at once.
Conclusion: Turn the chart into a protocol you can actually execute
A strong best peptide stack cjc 1295 ipamorelin bpc 157 tb 500 aod 9604 dosage protocol isn’t about chasing one “perfect” number—it’s about protocol logic: goal alignment, controlled sequencing, consistent administration, and honest tracking. That’s what turns a multi-peptide plan from speculation into an experiment you can learn from.
Next step: Create your protocol worksheet using the table in this guide, pick one primary goal, and decide whether you’ll run CJC-1295 + Ipamorelin first (or stagger tissue-support peptides) before adding AOD-9604—then track sleep, recovery, and injection-site comfort for your evaluation window.
Discussion