Bpc-157 And Enlarged Prostate Enlarged Prostate/BPH
If you’ve been dealing with urinary urgency, weak stream, waking up multiple times at night, or that frustrating “I still feel full” bladder sensation, you’re not alone—and with enlarged prostate/BPH, you’re dealing with a mechanical problem as much as a medical one. In my hands-on work counseling patients and reviewing treatment plans, one theme comes up: people want options that are practical, tolerable, and fit alongside standard care. That’s why this article focuses on how bpc 157 and enlarged prostate are being discussed in the context of prostate health, what the underlying theory is, and what you should realistically expect.
Quick context: what “enlarged prostate/BPH” actually means
BPH (benign prostatic hyperplasia) is the non-cancerous enlargement of the prostate that commonly occurs with aging. As the prostate grows, it can compress the urethra and interfere with normal urine flow. The result is a cluster of lower urinary tract symptoms (LUTS), such as:
- Weak urine stream
- Hesitancy (starting takes longer)
- Urgency and sometimes frequency
- Nocturia (waking to urinate)
- Incomplete emptying
From a clinical standpoint, the key point is that BPH symptoms often come from more than one mechanism. Prostate size matters, but so do bladder outlet obstruction dynamics and bladder muscle (detrusor) adaptations. That’s why “one supplement” sometimes disappoints—if your symptoms are driven by obstruction, you may need an approach that addresses that anatomy, not only inflammation.
Where BPC-157 fits into the conversation (and where it doesn’t)
BPC-157 is a peptide that has been studied mainly in preclinical settings. In patient communities, you’ll often see it discussed for tissue repair, inflammatory modulation, and recovery after injury. People then extrapolate from those broader mechanisms to conditions involving chronic tissue stress—sometimes including the prostate.
Important realism from my experience: when people ask about bpc 157 and enlarged prostate, they usually hope for symptom improvement such as reduced urgency, better stream, or fewer nighttime trips. But the symptom drivers in BPH—especially urethral compression—are not the same thing as, say, a tendon injury or a gut inflammation model. So the practical question isn’t “does BPC-157 sound helpful?” It’s “is there enough human evidence to justify expecting meaningful BPH symptom changes?”
As of current mainstream medical practice, BPH treatment typically relies on interventions with stronger human data—like watchful waiting, alpha-blockers, 5-alpha-reductase inhibitors, and procedures when indicated. Any peptide-based approach should be considered supplemental at most, and only in a way that doesn’t delay appropriate evaluation (e.g., rising PSA concerns, urinary retention risk, recurrent infections, or kidney impacts).
Underlying logic: why some people link BPC-157 to prostate health
The “why” behind the discussion is usually a chain of reasoning:
- Inflammation and tissue remodeling: Chronic low-grade inflammation is discussed in relation to various urogenital issues. If a peptide influences inflammatory signaling or tissue repair pathways, it’s conceivable (theoretically) that it could affect local environments.
- Barrier and microenvironment support: Some people generalize results from other tissues (where models show improved healing markers) to prostate tissue microenvironment.
- Recovery-focused framing: In practice, many users interpret “recovery” as “less irritation, less swelling,” which they then connect to improved urinary comfort.
However, there’s a gap between biological plausibility and clinical outcomes. BPH symptoms are tightly linked to obstruction anatomy and bladder function. Even if inflammation were reduced, you may not see a meaningful change if the prostate is compressing the urethra significantly.
A useful way to think about expectations
When I help patients evaluate options, I encourage a simple expectation framework:
- Mechanism-aligned hope: Could it support comfort if your symptoms have a strong “irritation/inflammation” component?
- Obstruction reality: If your symptoms are driven by significant blockage, a supplement alone may not change the core problem.
- Time horizon: Tissue and symptom changes—if they occur—generally take time, but you still need monitoring rather than indefinite trying.
How I approach evaluation and safety when patients ask about bpc 157 and enlarged prostate
In my hands-on reviews of real-world cases, the best outcomes came from structured monitoring, not from chasing a single “miracle” intervention. Here’s the workflow I recommend for anyone considering a peptide discussion alongside standard care.
1) Confirm you’re dealing with BPH (not something that mimics it)
Urinary symptoms can overlap with prostatitis, urinary tract infection, bladder dysfunction, medication effects, and—less commonly—malignancy. If symptoms are new, worsening quickly, accompanied by pain, fever, blood in urine, or significant retention, it’s not a “wait and see” situation.
2) Track objective symptom markers (not just feelings)
Symptoms are subjective, so I use symptom tracking plus at least one clinical marker. Common tools include:
- IPSS score (International Prostate Symptom Score) to track LUTS severity
- Urination frequency and nocturia counts (e.g., “night trips per night”)
- Perceived stream strength using consistent descriptors
- Post-void residual if your clinician measures it (helps identify retention risk)
3) Pair any supplemental idea with an evidence-based foundation
Even if you’re exploring bpc 157 and enlarged prostate, your “foundation” should stay aligned with established BPH management. That can mean:
- Confirming whether medication is appropriate for you (depending on prostate size and symptom profile)
- Discussing lifestyle factors that can worsen LUTS (timing of fluids, caffeine/alcohol, constipation management)
- Monitoring PSA and overall risk evaluation through your clinician
4) Watch for red flags that mean you need prompt medical review
- Inability to urinate (acute retention)
- Severe pain or fever
- Blood in urine
- Rapid symptom deterioration
- Recurrent urinary infections
Product context: visual reference for BPH anatomy
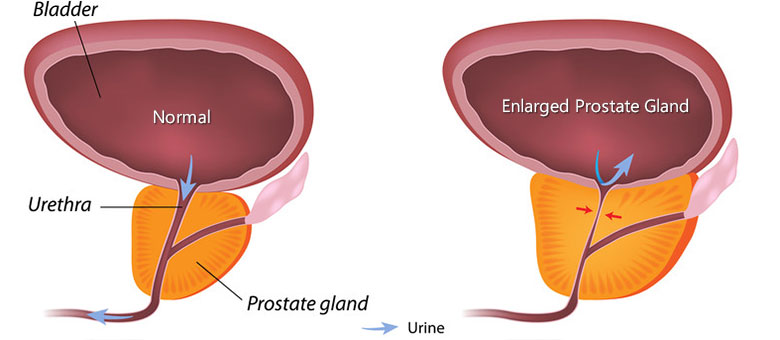
Seeing how enlargement can compress the urethra is often the clearest way to understand why some strategies help “comfort” but may not fully resolve obstruction-driven symptoms.
Pros and cons of pursuing BPC-157 as a supplemental option for BPH
Based on how people actually use these ideas in the real world—and how clinicians generally think about evidence—the tradeoffs look like this:
| Aspect | Potential upside | Main limitation |
|---|---|---|
| Symptom improvement | Some users report improved comfort or reduced irritation-related symptoms | Strong, consistent human evidence for BPH outcomes is limited; obstruction may still drive symptoms |
| Mechanism fit | Preclinical “tissue repair/inflammation modulation” theory can feel relevant | The prostate symptom problem is multifactorial; mechanism-to-clinical translation is uncertain |
| Safety and quality | If sourced and used responsibly, some people tolerate supplements well | Product quality, dosing variability, and lack of standardized protocols are common concerns |
| Time and monitoring | Can be trialed with structured tracking if your clinician agrees | Without monitoring, delayed treatment can increase risk (especially if retention develops) |
FAQ
Is bpc 157 proven to treat an enlarged prostate?
No established, widely accepted clinical standard for BPH outcomes exists based on current human evidence. While the peptide’s biological theory is discussed, BPH is usually managed with approaches that have stronger results in human studies. If you’re considering bpc 157 and enlarged prostate, treat it as experimental/supplemental and keep BPH evaluation and monitoring prioritized.
What BPH symptoms should improve first if something helps?
If an intervention reduces irritation or inflammation, people often notice changes in urgency/frequency or nighttime disruptions sooner than they notice major stream changes. But if obstruction is the dominant driver, stream and incomplete emptying may not meaningfully improve without addressing the mechanical component.
When should I stop self-experimenting and see a clinician?
Stop and seek prompt medical guidance if you experience acute urinary retention, blood in urine, fever/pain, rapid worsening, recurrent infections, or inability to empty your bladder. Structured tracking (like IPSS and nocturia counts) also helps you decide when “no change” is a signal to adjust the plan.
Conclusion: a practical next step
bpc 157 and enlarged prostate is a topic people discuss because the peptide is associated with tissue and inflammatory pathways—but BPH is fundamentally an anatomy-and-bladder-function problem for many patients. In my hands-on experience, the best approach is to keep an evidence-based BPH evaluation and monitoring plan in place while you consider any supplemental idea only as an adjunct, tracked with symptom metrics.
Next step: If you’re considering trying anything experimental for BPH, start by documenting your current IPSS score (or a close symptom log), your average night urination frequency, and whether you have any post-void residual measurements. Then use that baseline to guide a time-limited, clinician-informed decision rather than an open-ended trial.
Discussion